

Infant formulas: a good idea?
You've already guessed my answer, haven't you? Indeed, it's not a good idea :(
Mind you, I don't want to cast stones at those who choose not to breastfeed. What's more, although I don't think a young mother should have to justify her decision, there are cases in which breastfeeding is not advisable or simply not possible. It's rare, but there are, for example, hormonal pathologies that make breastfeeding difficult. There are also contraindications, such as taking certain medications or metabolic diseases in infants. And there are all those cases where breastfeeding is simply too painful, and you have to throw in the towel.
Not breastfeeding is not a catastrophe. But it is important to choose the right infant milk.
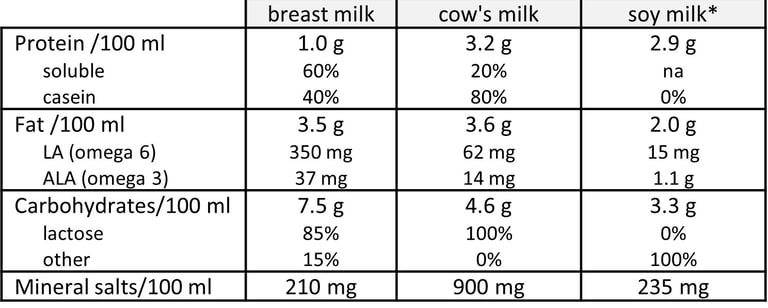
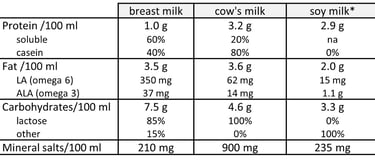
First of all, in case you've had the idea, forget animal milk (cow's or any other animal's) and forget vegetable milk (e.g., soy, rice) to feed a baby. Their composition is simply not adapted to baby's needs! I repeat: don't use animal or plant milk to feed a baby, as their composition is simply not adapted to its needs. In the case of animal milks, the ratio of casein to lactoferrin is unsuitable and increases the risk of allergy, while the high calcium and potassium content may overload the baby's kidneys. From a nutritional point of view, they also contain too many proteins and minerals, not enough carbohydrates, and their fatty acid composition does not correspond to baby's needs. Vegetable milks, on the other hand, are not rich enough in lipids and carbohydrates, and contain neither lactose nor casein. Here's a comparison between breast milk, cow's milk and soya milk (for the latter, I've based myself on averages, as its composition is not standardized):
As for infant formulas, the pediatrician may say that they all have to comply with the relevant legislation and are therefore perfectly safe. I think it's important to qualify this statement. It's true that they must comply with legislation aimed at optimizing their composition, by setting minimum and maximum contents in nutrients. The legislation is different in the US and in Europe. I’m here detailing the US specificities. For the European ones, please refer to the French version of this article. The US legislation sets minimum and maximum contents in proteins, lipids (including AL), vitamins (A, D, E, K, B1, B2, B3, B5, B6, B8, B9, B12, C), minerals (calcium, phosphorus, magnesium, iron, zinc, manganese, copper, iodine, selenium, sodium, potassium and chloride), choline (assimilated to vitamin B4) and inositol (assimilated to vitamin B7). I personally find it suboptimal that there are no requirements for carbohydrate content, nor excluded nutrients. That said, among the products on the market, which in principle comply with the legislation, I encourage you to choose according to the following criteria:
The ratio of casein to whey protein should be as close as possible to 30/70, which is that of breast milk. Whey proteins include lactoferrin, which is very important for immunity through its bacteriostatic (inhibits bacterial multiplication) and bactericidal (kills bacteria) action. On proteins, the legislation says “Protein shall be present in an amount not to exceed 4.5 g per 100 kcal regardless of quality, and not less than 1.8 g per 100 kcal when its biological quality is equivalent to or better than that of casein. If the biological quality of the protein is less than that of casein, the minimum amount of protein shall be increased proportionately. For example, an infant formula containing protein with a biological quality of 75% of casein shall contain at least 2.4 g of protein (1.8/0.75). No protein with a biological quality less than 70% of casein shall be used”.
Protein content should not exceed 1.5 g/100 ml (the legislation imposes a minimum content of 1.8 g/100 kcal and a maximum of 4.5 g/100 kcal, as we’ve just seen, which cannot be directly transposed into g/ml without knowing the nutritional composition of the infant formula concerned[1]).
The only carbohydrate present should be lactose. The legislation does not set any requirement about carbohydrate content and infant formulas may contain any approved carbohydrate sources: lactose, but also maltodextrin, corn syrup, brown rice syrup, corn syrup solids, and/or sucrose, which all bring potential issues.
Lipids should make up between 45 and 50% of energy intake (the legislation requires a minimum of 30% and a maximum of 54%).
The formula should be enriched with pre- and probiotics[2].
Enrichment with HMO prebiotics (breast-milk oligosaccharides, e.g., 2'-fucosyllactose) is also beneficial.
Note that infant formulas available in the U.S. must be labeled as either “infant formula with iron” or “additional iron may be necessary.” Formulas with iron are recommended to prevent iron-deficiency anemia.
Infant formulas are intended for children up to 12 months of age. Toddler nutritive drinks, often marketed as “toddler formulas,” are not necessary to meet the nutritional needs of older babies. Additionally, they do not undergo premarket review by FDA.
In addition to regular infant formulas, there are also formulas with specific indications, such as i) partially hydrolyzed formula containing cow’s milk proteins that have already been partially hydrolyzed, or broken down, to ease the digestion for infants suffering from colic, ii) spit-up formulas, that are thickened with the aim of reducing acid reflux and iii) lactose-free formula, for infants that have difficulty digesting it. If an infant suffers from reflux or colic, I advise you to first assess whether the problem is due to taking too much too quickly, taking too much, or holding the baby by compressing the stomach. Beware also that anti-reflux formulas are either thickened, often with carob flour (which can, in rare cases, provoke an allergy), or contain a substance that thickens on contact with gastric acidity. These products are even more processed than regular formulas.
There are also specialty formulas for infants with unusual medical or dietary problem, such as i) hypoallergenic formulas with extensively hydrolyzed proteins, for infants with milk protein allergy, ii) formulas for infants with Phenylketonuria, which do not contain the amino acid phenylalanine and iii) formulas for premature infants, which include more nutrients and calories than regular formulas.
I recommend using glass baby bottles. Plastic bottles should not be heated or contain hot milk (risk of releasing toxic substances and endocrine disruptors). Milk can be heated to around 37°C or 98.5°F. Do not heat it any higher than this to then leave it to cool, as milk heated to over 50°C or 122°F will have an increased carboxymethyl lysine content (an advanced glycation product), especially as it already contains some, having undergone high-temperature treatment during production. Lastly, the water added to dehydrated milk must have a low mineral content, so as not to overload the infant's kidneys.
To find out more, also read these articles:
On nutrition and supplements during pregnancy: https://isabellemaesnutrition.com/en/pregnancy
On the links between fertility and diet: https://isabellemaesnutrition.com/en/fertility
[1] Example of a calculation: let's imagine a formula containing 1.5 g protein, 4 g fat and 4 g carbohydrates in 100 ml. Knowing that there are 4 kcal in 1 g of carbohydrate and protein and 9 kcal in 1 g of fat, 100 ml of this formula contain 44.7 kcal. The protein content per 100 kcal is thus 7.4 g.
[2] Caution: for premature babies, probiotics must be taken under medical supervision, as their immunity is weak (risk of bacteremia).
Baby picture by Kelly Sikkema

